
In 2006, Dutch home care had a widely recognised problem. Nurses were calling in sick en masse. Patients saw an average of thirty different carers per year. Waiting lists grew. And despite years of budget cuts and reorganisations, costs kept rising.
The prevailing diagnosis: too little budget, too much demand, not enough staff. The prevailing response: more measurement, more protocols, more management. Jos de Blok, after 25 years as a nurse and manager in the sector, had a different diagnosis. The people were fine. The system was broken.
In 2007 he founded Buurtzorg with four nurses in Almelo. No managers, no timed task slots, no stacks of paperwork. Small self-managing teams of 10-12 nurses with full autonomy over their own neighbourhood.
Seventeen years later, Buurtzorg has 14,000 nurses across 950 teams, operating in 24+ countries. Ernst & Young calculated that if all Dutch home care adopted the model, it would save €2 billion per year in care hours.1
This article is a Buurtzorg case study through the behavioural design lens. Not another description of self-managing teams, but an analysis of exactly what Jos de Blok did, why it worked, and what any leader can learn from it.
What came before Buurtzorg: a system that made good behaviour impossible
To understand the Buurtzorg case, you need to know what Dutch home care looked like before Buurtzorg existed.
In the early 1990s, the government introduced New Public Management into healthcare. The intention: efficiency through standardisation. In practice, every care task became a separate "product" with a precise time allocation. Every step had to be logged to the second. External bodies determined which nurse was allowed to perform which tasks.
A decade later, the sector looked like this:
- Patients saw an average of thirty different carers per year, with no continuity
- Nurses worked in time slots of seven to fifteen minutes per task
- Every minute had to be tracked and invoiced
- Professional decision-making space was virtually zero
- Sector absenteeism: 10.4%
The irony: costs rose despite all the austerity intent. Long-term care expenditure grew from 2.8% to 4% of GDP between 1996 and 2005.2
For ten years the sector tried to fix this with more training, better protocols and stricter supervision. Nothing worked, because the diagnosis was wrong. It was not a motivation problem. Nurses had the motivation already, they brought it when they chose this profession. It was a context problem: the organisational structure made good work structurally impossible.
In behavioural science, this is called the Fundamental Attribution Error: we attribute failing behaviour to personality traits or motivation, while the situation is almost always the determining factor. The sector saw nurses burning out and thought: lack of resilience. The correct diagnosis was: a system that systematically destroyed resilience.
"I don't motivate my staff. I think doing that is too patronizing." - Jos de Blok
The insight: behaviour doesn't change by changing people
Jos de Blok never took a course in behaviour change. But his reasoning was exactly what behavioural science describes as the most underestimated principle in organisational design: people display the behaviour that their environment makes possible for them.
If the environment treats professionals as executors of protocols, they behave as executors of protocols. If the environment treats professionals as skilled decision-makers, they behave as skilled decision-makers. Not because management enforces it, but because that is the path of least resistance that the context has created.
The man who built the most engaged care organisation in the Netherlands does not believe in employee motivation as a management task. "I don't motivate my staff," he said in an interview. "I think doing that is too patronizing."
His intervention strategy was the precise opposite of what the sector had been trying for years. No better training, no new competency profiles, no communications campaign about values. Just this: remove the barriers that block good behaviour.
This is the central insight of Behavioural Design and simultaneously the most underestimated insight in leadership development. When behaviour doesn't change, managers almost automatically look for motivation problems. In reality, they are almost always capability problems - in SWAC terms: not a WANT deficit but a CAN deficit. And CAN problems are solved by removing barriers, not by motivating harder.
 Amsterdam City Centre
Amsterdam City Centre
The Influence Framework analysis: four forces reversed
When you apply the SUE Influence Framework to the Buurtzorg case, you see how the old system produced the wrong behaviour on all four forces, and how Buurtzorg reversed each one individually.
The desired behaviour: a nurse who delivers holistic, effective care that helps the patient become as independent as possible.
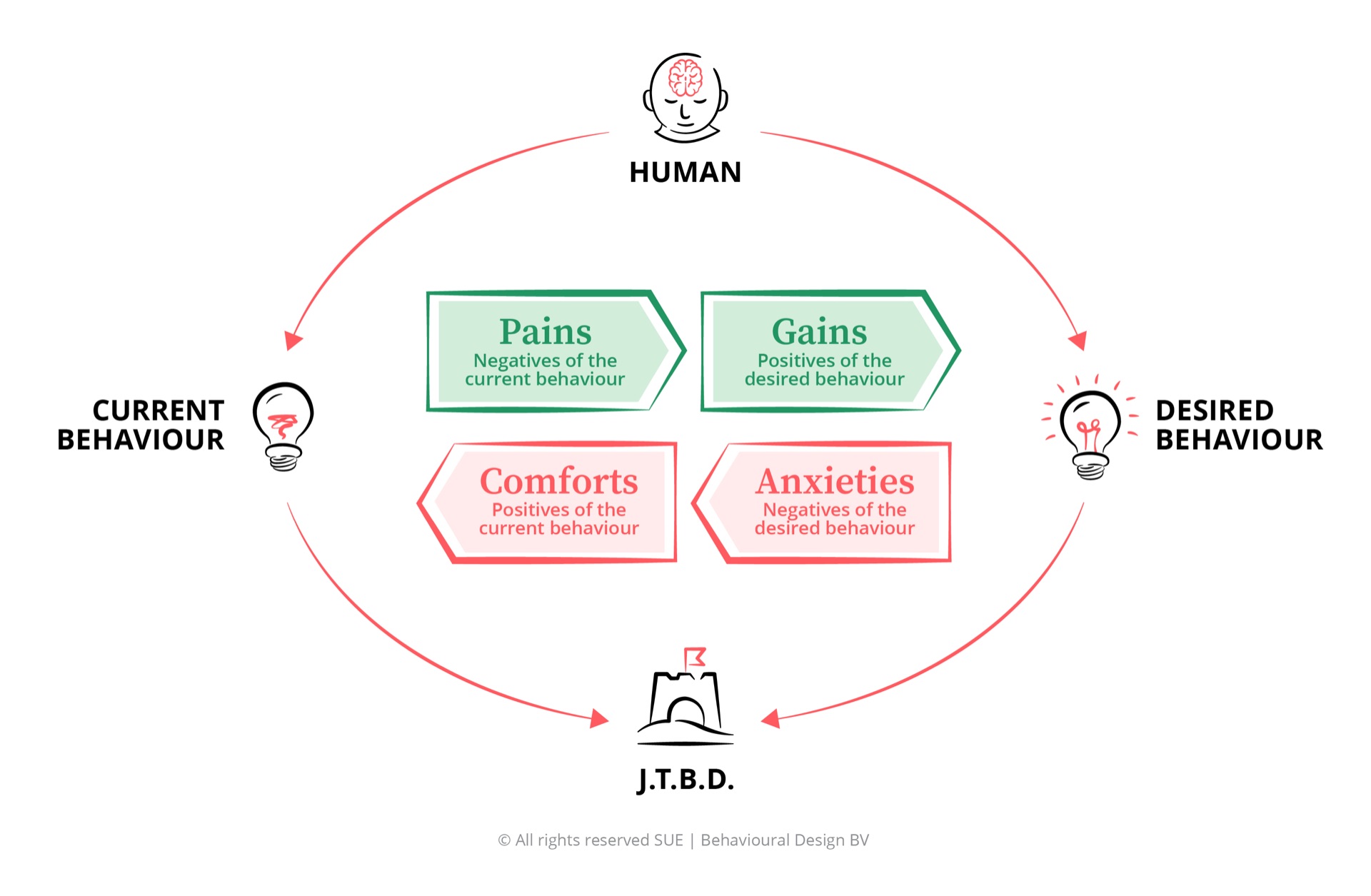
Pains resolved. No more time slots, no minute-by-minute logging, no thirty colleagues per patient. The daily frustration of meaningless work disappeared because the work itself became meaningful again.
Gains restored. Buurtzorg nurses care for each patient with 3-4 regular colleagues over a longer period. That continuity makes real relationships possible. Relationships are, for most nurses, exactly the reason they chose this profession. The intrinsic gain, the feeling that your work genuinely matters, had been protocolled away in the old system. Buurtzorg brought it back.
Anxieties removed. Teams make decisions they are professionally trained for. Buurtzorg explicitly selects on qualifications above the sector standard. The anxiety about making a "wrong" clinical decision in a micromanaged system disappeared, because the micromanagement disappeared.
Habits replaced. In the absence of managers, teams built their own working routines: consent-based decision-making, peer review, peer coaching. BuurtzorgWeb, an internal platform, made knowledge sharing the default. Social proof took over the role of hierarchical control: teams could see how other teams were performing and asked them directly for advice.
You're reading about it. But what if you could apply it yourself, to leaders, teams or stakeholders?
As Europe's #1 academy in Behavioural Design, we train professionals in analysing, predicting and influencing behaviour, live, online or in-company. Based in Amsterdam, with more than 10,000 alumni from London to Sydney.



 EQAC
EQACCertified
Training
Three design choices that carry the model
1. Self-direction with one hard boundary
The most radical choice Buurtzorg made is also the most misunderstood. No managers does not mean: everyone does whatever they want. It means: decision responsibility lies with the people who have the most information about the situation.
A Buurtzorg team of 10-12 nurses manages everything: patient intake, schedules, holiday planning, finances, hiring, office rental. There is one hard boundary: at least 61-62% of working time goes to direct patient care. Beyond that: full autonomy.
The 18-20 regional coaches who support all 950 teams have no authority over teams and carry no performance responsibility. They offer advice when asked, nothing more.
From a SWAC perspective, this is a precisely designed system. The CAN problem was solved by selecting nurses on higher qualifications than the sector standard and by placing decision-making space directly with them. The WANT problem never existed, the system had simply blocked it. The SPARK and AGAIN were secured by the structure of small teams with shared responsibility for their own neighbourhood.
Deci and Ryan's self-determination theory offers an explanation here.3 People have three fundamental psychological needs: autonomy (control over one's own actions), competence (growing in expertise) and relatedness (meaningful relationships). The old home care system destroyed all three. Buurtzorg restored all three. The results are the outcomes the theory predicts. You don't need to call it a miracle once you understand the mechanisms.
2. BuurtzorgWeb: transparency as a behaviour driver
Buurtzorg has no HR department, no planning department, no marketing department. What it does have is BuurtzorgWeb: an internal platform where teams share knowledge in real time, compare performance and solve problems.
A nurse facing a difficult situation posts a question. Within hours, colleagues from across the country respond. Financial performance is visible to every team, including how they score against other teams.
This is a deliberate choice for peer accountability over hierarchical control. Social comparison is a powerful behaviour driver. By making performance transparent, "how are other teams doing this well?" became the natural reference question, not "what does the protocol say?". The norm was created by visibility, not by rules.
The platform is estimated to save 20% on administrative costs compared to traditional systems. But the behavioural effects run deeper: it makes knowledge sharing the default route and hierarchical approval the exception.
3. The Onion model: patient autonomy as the design goal
Buurtzorg's care philosophy works like an onion. At the centre: the patient and their own capacity for independence. The second layer: the informal network of family, neighbours and community associations. Only then comes the nurse. The fourth layer is the broader professional network.
The nurse always starts at the centre: what can this person do themselves? What can their environment support? Only when those layers are insufficient does professional care expand outward.
This inverted the dominant care model. Traditional home care started with the care task and worked down to the patient. Buurtzorg starts with the person and works up to the care task when necessary. The behavioural economics implication: by making autonomy the design goal rather than maximising care consumption, an entirely different patient behaviour emerges. Buurtzorg patients use an average of 108 care hours per year, versus 168 at other providers.1
The results: what happens when you change the context
The Buurtzorg case study produces a set of figures difficult to match anywhere in the organisational literature:
- Absenteeism: roughly half the sector average (sector: 10.4%)
- Turnover: 10% versus 15% nationally
- Patient satisfaction: 9.1 out of 10, 30% above the national average
- Care hours per patient per year: 108 versus 168 at other providers (Ernst & Young, 2009)
- Overhead: 8% versus 25% sector average
- Employee engagement: 9.5 out of 10 (Effectory)
- Best Employer Netherlands: four times elected by Effectory (2011, 2012, 2014, 2015)
KPMG confirmed in 2015, commissioned by the Ministry of Health, that Buurtzorg is a low-cost provider even when accounting for the higher hourly wages the organisation pays. Adjusted for patient mix, total care costs per patient were 3% below average.4
And then the number rarely mentioned: all of this is managed by 50 headquarters staff and 18-20 coaches for 950 teams and 14,000 nurses.
There are no managers. These are the results.
The explanation you hear most often: "It works because nurses are intrinsically motivated." That explanation is correct, but it entirely misses the point. The nurses in the old system were also intrinsically motivated. They consciously chose this profession. The system systematically destroyed that motivation. Buurtzorg did not create the motivation. It removed the context that was destroying it.
What this means if you are a leader
The temptation is to dismiss Buurtzorg as a special case in a special sector. That temptation is understandable, but the behavioural principles behind the model are not sector-specific.
Three questions the Buurtzorg case study poses to every leader:
What are we measuring, and what are we measuring away?
The NPM system measured minutes per task. In doing so, it measured away: continuity, professional judgement, prevention, patient relationships. Every measurement system reinforces certain behaviour and makes other behaviour invisible. The question is not whether you measure something, but which behaviour you unintentionally measure away when you do.
In organisations outside healthcare, we see the same pattern. Teams evaluated on speed optimise for speed, even when that costs quality. Employees evaluated on presence optimise for presence, even when that costs productivity. The metrics determine behaviour, not the values on the wall.
Do our processes treat people as professionals or as executors?
Every approval process, every mandatory report, every control protocol is a signal. It implicitly says: we don't trust your judgement here. That signal has consequences for how people behave, regardless of what you formally expect.
Behavioural science calls this self-determination theory: people who feel their autonomy is undermined display less ownership, less initiative and less problem-solving behaviour. Not because they are lazy, but because the context teaches them to be.
Where does the real problem lie?
When behaviour doesn't change, managers almost automatically look for motivation problems: more communication, better incentives, inspiring sessions about vision and values. Buurtzorg shows that the problem in most cases lies in the structure. In information flows. In the decision-making space people do or do not have. These are CAN problems, and you solve them by removing barriers, not by turning up the motivation dial.
If you ask employees why they don't display certain behaviour and they answer "that doesn't work in this system" or "I don't have time for that" or "that always has to go through a manager", you have a CAN problem. The solution is not a training programme. The solution is adjusting the system.
Want to read more about how to map behavioural barriers in organisations? Also read Change management as behavioural design and How ING turned 3,500 employees into self-organising teams.
Frequently asked questions about the Buurtzorg case study
Buurtzorg works not because nurses are intrinsically motivated - they were before Buurtzorg too. It works because Buurtzorg removed the context that made good behaviour impossible. Self-managing teams, no time slots, real patient relationships and peer accountability via BuurtzorgWeb removed exactly the barriers that the old home care system had erected.
Start by asking: which parts of our organisational structure make desired behaviour harder than undesired behaviour right now? The Buurtzorg lesson is not "abolish managers", but "audit the barriers in your system". Every approval process, every mandatory report and every measurement system is a potential behavioural barrier.
Absenteeism roughly half the sector average, turnover 10% versus 15% nationally, patient satisfaction 9.1 out of 10, care hours per patient 108 versus 168 at other providers, overhead 8% versus 25% average. Ernst & Young calculated that national adoption of the model would save €2 billion per year in care hours. Four times elected Best Employer of the Netherlands (Effectory, 2011-2015).
The behavioural principles behind Buurtzorg are not sector-specific. The combination of autonomy, craftsmanship and peer accountability works in any organisation where people do professional work. The model is now applied in 24+ countries and across various sectors outside healthcare.
A motivation problem means people don't want to show the desired behaviour. A CAN problem means people cannot show the desired behaviour because of context or structure. In the Buurtzorg case there was no motivation problem: nurses consciously chose this profession. It was a CAN problem: the organisational structure made good care structurally impossible.

1.5 minutes of Influence
Every week I notice something: a hospital sign, a supermarket shelf, a phrase in a meeting. Always something that shows exactly how context shapes behaviour. I write it down. Every Thursday morning it lands in your inbox. In 90 seconds.
Read by 10,000+ professionals from 45+ countries · Free · Unsubscribe anytime

